8 Topic: Community Violence
Learning Outcomes
- Analyze the multifaceted nature of community violence.
- Identify risk factors and warning signs associated with various forms of community violence.
- Evaluate the impact of community violence on individuals, families, and communities, and analyze the role of healthcare professionals and community organizations in addressing and preventing violence.
Violence is a critical health problem that has become pervasive throughout the United States. The World Health Organization (WHO) Violence Prevention Alliance has defined violence as “the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, that either result in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation” (WHO, 2021).
Violence affects millions of people, and their families, schools, and communities every year. Violence can cause significant physical injuries and mental health conditions such as depression, anxiety, and posttraumatic stress disorder (PTSD). Living in a community experiencing violence is also associated with an increased risk of developing chronic diseases. Concerns about violence may prevent some people from engaging in healthy behaviors, such as walking, bicycling, using parks and recreational spaces, and accessing healthy food outlets (CDC, 2022e).
Violence
Violence is not an individual issue but a societal and global concern. Social justice cannot be ensured as long as the threat of violence exists. According to Healthy People 2030, objectives to address crime and violence include reducing:
- The rates of minors and young adults committing violent crimes
- Nonfatal physical assault injuries
- Firearm-related deaths
- Adolescent sexual violence by anyone
- Sexual or physical teen dating violence
- Bullying of lesbian, gay, or bisexual high school students
- Domestic and Intimate Partner Violence
Domestic and Intimate Partner Violence
The National Coalition Against Domestic Violence (NCADV) defined domestic violence as “the willful intimidation, physical assault, battery, sexual assault, and/or other abusive behavior as part of a systematic pattern of power and control perpetrated by one intimate partner against another. It includes physical violence, sexual violence, threats, economic abuse, and emotional/psychological abuse. The frequency and severity of domestic violence vary dramatically” (WHO, 2021). Furthermore, domestic violence does not discriminate. More than 80 million people in the United States have experienced IPV in their lifetime (California Firearm Violence Research Center, 2022).
Although the terms domestic violence and intimate partner violence are sometimes used interchangeably, the distinction exists in the sense that domestic violence can occur between a parent and child, siblings, or roommates. Intimate partner violence occurs between romantic partners who may or may not be living together in the same household (CDC, 2024e).
Intimate partner violence can exist in all relationships and at every level, including between those who are married or are dating, living together, or encountering each other after the relationship has ended (Kang et al., 2017). Intimate partner violence is a persistent problem. Approximately two in five women and nearly one in four men have experienced contact sexual violence, physical violence, and/or stalking by an intimate partner during their lifetime and have reported some form of IPV-related impact. Over 61 million women and 53 million men have experienced psychological aggression by an intimate partner in their lifetime (CDC, 2024e). Every year, 3–4 million women in the United States. are abused, and 1,500–1,600 are killed by their abusers.

Risk factors for experiencing IPV are considered from the perspective of an individual in the context of relationship, community, and societal factors. Examples of risk factors include low self-esteem, aggressive or delinquent behavior as a youth, witnessing violence between parents as a child, communities with high unemployment rates, and societal income inequality (CDC, 2024). Intimate partner violence often begins early and continues throughout the lifespan. When IPV occurs in adolescence, it is called teen dating violence. Teen dating violence affects millions of U.S. teens each year. Approximately 11 million women and 5 million men who reported experiencing contact sexual violence, physical violence, or stalking by an intimate partner in their lifetime said that they first experienced these forms of violence before age 18 (CDC, 2024e). Data from the CDC’s Youth Risk Behavior Survey in 2019 indicated that among U.S. high school students who reported dating during the 12 months before the survey, about one in 12 experienced physical dating violence. About one in 12 of the surveyed high school students experienced sexual dating violence (CDC, 2024e).
Intimate partner violence is preventable. A number of factors may increase or decrease the risk of perpetrating and experiencing IPV. Nurses can play a role in helping to reduce and prevent IPV by doing the following:
- Understanding the risk factors for experiencing violence and identifying protective factors.
- Promoting healthy, respectful, and nonviolent relationships. Nurses can model this through therapeutic communication and through sharing resources that help individuals and couples develop healthy and safe relationships.
- Seeking additional training to understand the shared risk and protective factors. Since addressing and preventing one form of violence may have an impact on preventing other forms of violence, nurses can significantly influence violence reduction and prevention.
- Referring persons experiencing IPV to the domestic violence website and hotline are among other resources that should be offered to persons in this situation. The domestic violence hotline is a shareable resource for people who are affected by IPV (National Domestic Violence Hotline, 2022).
| Healthy Relationships | Unhealthy Relationships |
| Equality: You make decisions together. | Control: One of you makes all the decisions and is demanding. |
| Honesty: You can share your feelings and thoughts with each other. | Dishonesty: One of you lies and hides things from the other. |
| Physical safety: You feel safe with each other. You are not scared of getting hurt. | Physical abuse: One of you hits, slaps, grabs, or shoves the other person. |
| Respect: You respect each other’s opinions, friends, and interests. | Disrespect: One of you makes fun of the other’s feelings, thoughts, and opinions. |
| Comfort: You feel great being yourself, and you are comfortable saying “I am sorry.” | Discomfort: One of you might make threats like “I will break up with you if. . . ” |
| Sexual respectfulness: You never force each other to do things you are uncomfortable with. | Sexual abuse: One of you pressures the other or forces sexual activities the other does not want to do. |
| Independence: You have friends and hobbies outside your relationship. | Dependence: One of you makes threats to do something drastic if the relationship ends. |
| Humor: You have fun in the relationship. | Hostility: One of you is mean to the other. |
An in-depth assessment of the person suffering IPV must be undertaken and a safety plan developed. Establishing a plan does not necessarily mean that the person experiencing the violence is willing and able to leave at that time. The goal is to support the patient’s decision, offering support, resources, and contact information if desired.
Protective Factors for Intimate Partner Violence Perpetration
Relationship Factors
The following are relationship factors community and public health nurses need to consider when addressing the needs of individuals at risk for IPV:
- Strong social support networks and stable, positive relationships with others
- Support groups for single, divorced, or separated individuals at risk for IPV
- Screening and referral of individuals acknowledging significant relationship discord
- Screening and referral of individuals expressing impactful relationship satisfaction
- Identification and referral of individuals demonstrating attachment disorders from their adult partners
- Referral of individuals expressing significant emotions of anger and jealousy toward their partner (Capaldi et al., 2012)
Community Factors
Community factors that may help them serve the needs of persons at risk for IVP. Community health nurses should consider these factors:
- Neighborhood collective efficacy (i.e., residents feel connected to each other and are involved in the community)
- Coordination of resources and services among community agencies
- Access to safe, stable housing
- Access to medical care and mental health services
- Access to economic and financial help
LGBTQIA+ Violence
Homophobia, stigma, and discrimination increase the chance for individuals of the lesbian, gay, bisexual, transgender, questioning/queer, intersex, and asexual (LGBTQIA+) community to experience violence. Violence can include behaviors such as bullying, teasing, harassment, physical assault, IPV, and suicide-related behaviors. Several aspects of IPV can be unique to the LGBTQIA+ community (CDC, 2016). “Outing” or threatening to reveal one partner’s sexual orientation or gender identity may be used as a tool of abuse in violent relationships and may also be a barrier that reduces the likelihood of help-seeking for the abuse. Prior experiences of physical or psychological trauma, such as bullying and hate crime, may make persons who are LGBTQIA+ less likely to seek help (NCADV, 2018).
Types of Domestic Violence Affecting the LGBTQIA+ Community
Consider the following statistics:
- 20% of victims have experienced some form of physical violence
- 16% have been victims of threats and intimidation
- 15% have been verbally harassed
- 4% of survivors have experienced sexual violence
- 11% of intimate violence cases reported in the 2015 report by the National Coalition Against Domestic Violence Programs (NCADVP) involved a weapon (NCAVP, 2016)
The 2015 U.S. Transgender Survey found that more than half (54%) of transgender and non-binary respondents experienced IPV in their lifetimes. Nurses must understand that the community of LGBTQIA+ can experience bias from health care and law enforcement (CDC, 2022a). Many times, persons who are not cisgender are discouraged from seeking help for IPV. For many LGBTQIA+ people, IPV often begins in youth or young adulthood. One in five (19%) lesbian, gay, and bisexual high school-aged students have said they have been forced to have sex, compared with 6% of straight students (CDC, 2019). Another study found that nearly one in four (24%) transgender high school–aged students said they have been forced to have sex, as well as 15% of their cisgender peers. In addition, lesbian, gay, and bisexual high school–aged students report elevated rates of physical (13%) and sexual (16%) dating violence, compared with the rates of physical (7%) and sexual (7%) dating violence reported by their straight peers (CDC, 2019; Johns et al., 2019). Transgender students also report high levels of physical (26%) and sexual (23%) dating violence, compared with the rates of physical (15%) and sexual (16%) dating violence reported by their cisgender peers (Human Rights Campaign Foundation, 2022; Johns et al., 2019). Unfortunately, persons who are LGBTQIA+ experience health inequities and discrimination in the healthcare system.
Violence Against Children
Violence is a major public health and human rights concern. An estimated 1 billion children—half of all the children in the world—are victims of violence every year. Children who experience violence have higher risks for health and social problems, such as chronic disease, HIV, mental health issues, substance misuse, and reproductive health problems. Violence also leads to continued cycles of violence, because young people who experience violence are more likely to perpetrate violence against others later in life (CDC, 2024a).
Child abuse and neglect are common. At least one in seven children has experienced child abuse or neglect in the past year in the United States. This is likely an underestimate because many cases are unreported. In 2020 in the United States, 1,750 children died of abuse and neglect.
Children living in poverty experience more abuse and neglect than do those in households that are not impoverished. Experiencing poverty can place a lot of stress on families, which may increase the risk of child abuse and neglect. Rates of child abuse and neglect are five times higher for children in families with low socioeconomic status than for those in higher-status families.
Child maltreatment is costly. In the United States, the total lifetime economic burden associated with child abuse and neglect was about $592 billion in 2018. This economic burden rivals the cost of other high-profile public health problems, such as heart disease and diabetes (CDC, 2024c).
Long-term behavioral impacts of violence on children include aggressive and antisocial behavior, substance abuse, risky sexual behavior, and criminal behavior. Despite these grave physical and mental health consequences, most children who have been victimized by violent acts never seek or receive help to recover. Children who grow up with violence are more likely to reenact it as young adults and caregivers, creating a new generation of persons who have been abused (UNICEF, 2020).
School violence can seriously affect children’s psychological and physical health. Children who are subjected to violence may experience physical injury, sexually transmitted infections, depression, anxiety, posttraumatic stress disorder (PTSD), and suicidal thoughts. They may also begin to exhibit risky, aggressive, and antisocial behavior. Children who grow up around violence, compared with those who do not, have a greater chance of replicating it for a new generation of persons to be victimized. At its most extreme, violence in and around schools can be deadly. School often becomes the front line for the millions of children and adolescents living in conflict-affected areas. Violence in school can reduce school attendance, lower academic performance, and increase dropout rates. This result of school violence has devastating consequences for the success and prosperity of children, their families, and entire communities (UNICEF, 2021).
Strategies to Combat Childhood Violence
The CDC has recommended Essentials for Childhood to foster the positive development of children and families and, specifically, prevent all forms of child abuse and neglect. While each individual goal is important to community health, the four goals together are more likely to build a comprehensive foundation of safe, stable, nurturing relationships and environments for children. Community health nurse can promote the following strategies:
Goal 1: Raise awareness and commitment to promote safe, stable, nurturing relationships and environments and prevent child abuse and neglect
-
- Adopt the vision of “assuring safe, stable, nurturing relationships and environments to protect children from child abuse and neglect”
- Raise awareness in support of the vision
- Partner with others to unite behind the vision
Goal 2: Use data to inform actions
-
- Build a partnership to gather and synthesize relevant data
- Take stock of existing data
- Identify and fill critical data gaps
- Use the data to support other action steps
Goal 3: Create the context for healthy children and families through norms change and programs
-
- Promote the community norm that we all share responsibility for the well-being of children
- Promote positive community norms about parenting programs and acceptable parenting behaviors
- Implement evidence-based programs for parents and caregivers
Goal 4: Create the context for healthy children and families through policies
-
- Identify and assess which policies may positively affect the lives of children and families in your community
- Provide decision-makers and community leaders with information on the benefits of evidence-based strategies and rigorous evaluation (CDC, 2021)
Children who experience violence are at risk for long-term physical, behavioral, and mental health problems. Strategies to protect children from violence can help improve their health and well-being later in life (Office of Disease Prevention and Health Promotion, 2022). While child abuse and neglect are significant public health problems, they are also preventable (CDC, 2021).
Adverse Childhood Experiences
Adverse childhood experiences (ACEs) include child abuse and neglect but also encompass household events that children may experience as traumatic (Figure 7.3). The CDC–Kaiser Permanente ACE study is one of the largest investigations of childhood abuse, neglect, and household challenges. The study clearly linked ACEs and later-life health and well-being. The greater the culmination of ACEs, the poorer the health outcomes later in life (Felitti et al., 1998).

Why Are ACEs a Problem?
Adverse childhood experiences are violations of the safety and well-being of children. They also indicate a family structure in which children and adults are suffering. Moreover, the more ACEs a person experiences, the higher their risk for health-related issues such as these:
- Alcoholism
- Unplanned teen pregnancy
- Depression
- Diabetes
- Heart disease
- IPV
- Suicide
- Eating disorders
- Drug abuse
- Sexuality Transmitted Infections
Since the prevention of ACEs is important to the well-being of a vulnerable population (children) and families as well as to public health, the CDC has developed some research-based strategies to prevent ACEs and mitigate their impacts. Table 5 outlines strategies and approaches that public health nurses can facilitate through working with families and communities.
- Social-emotional learning
- Safe dating and healthy relationship skill programs
- Parenting skills and family relationship approaches
| Preventing Adverse Childhood Experiences | |
|---|---|
| Strategy | Approach |
| Strengthen economic support to families |
|
| Promote social norms that protect against violence and adversity |
|
| Ensure a strong start for children |
|
| Teach skills |
|
| Intervene to lessen immediate and long-term harms |
|
Human Trafficking
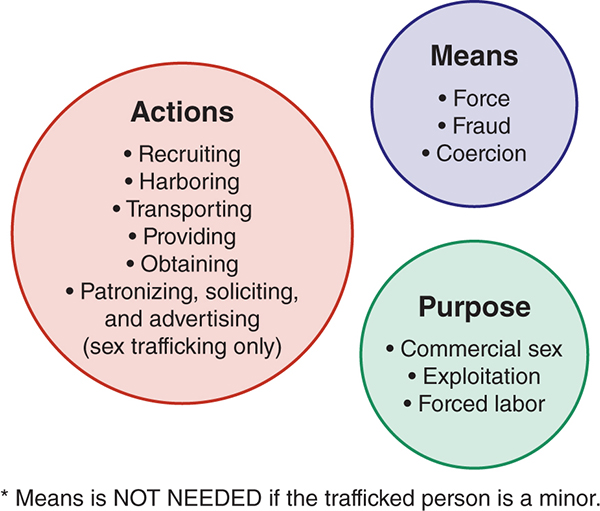
Human trafficking is also called “modern-day slavery” (U.S. Department of Health and Human Services, 2020). It involves the exploitation of people through force, coercion, threat, and deception and includes human rights abuses. The action means, and purposes model (AMP) describes the definition of human trafficking in the United States, as outlined by the Victims of Trafficking and Violence Protection Act of 2000. For something to be considered human trafficking, at least one item from each circle shown must be present; however, means is not necessary if the person being trafficked is a minor (National Human Trafficking Hotline, 2014). The A M P model of human trafficking describes the actions, means, and purpose.
Human trafficking is a human rights violation that denies individuals their basic freedoms and dignity. Human trafficking is underreported, underrecognized, and under-prosecuted. Currently, there is no national requirement for nurses to engage in annual or continuing education in assessing or reporting human trafficking. This is extremely concerning because 87% of trafficked persons said that while in captivity, they had interactions with a healthcare professional but their captivity went completely undetected (Farella, 2016). House Bill 2282 (February 24, 2017) mandated that the Department of Education develop guidelines for training school personnel. This bill includes the community health role of school nurses.
Understand that many trafficked persons believe that they will be prosecuted. However, U.S. law states that any crimes that occur during captivity are not considered criminal acts by the captive, only by the offender. Communicate early and often with your colleagues and manager to enlist help
Documentation
Document all the following in detail about the person who has been trafficked:
- Signs of physical abuse
- Signs of psychological abuse
- The trafficked person’s “story”
- Any laboratory results or assessments that support what your patient is telling you
- Also, document the following behaviors of the offender if they are present
- Not letting the patient speak for themselves
- Holding all currency and important documents
- Not allowing the trafficked person to be alone with the healthcare provider
Protection
Because one in every three trafficked persons is a child, nurses must understand reporting mandates. Nurses are legally mandated to report any suspicion of trafficking cases involving people under 18. However, there is no reporting mandate for adults who are trafficked. Nonetheless, nurses can still protect their patients by doing the following:
- Establishing an anonymous/protected status in clinics, primary care, and acute care settings
- Contacting local police
- Calling the National Trafficking Hotline at 1-888-373-7888
- Involving case management for after-care resources
Gun Violence
Gun violence is a serious public health problem that affects the health and safety of Americans. Important gaps remain in our knowledge about the problem and ways to prevent it. Addressing these gaps is an important step toward keeping individuals, families, schools, and communities safe from firearm violence and its consequences.
A firearm injury is a gunshot wound or penetrating injury from a weapon that uses a powder charge to fire a projectile. Weapons that use a power charge include handguns, rifles, and shotguns. Injuries from air- and gas-powered guns, BB guns, and pellet guns are not considered firearm injuries because these types of guns do not use a powder charge to fire a projectile.
Firearm injuries are a serious public health problem. In 2020, there were 45,222 firearm-related deaths in the United States—that is about 124 people dying from a firearm-related injury each day. More than half of firearm-related deaths were suicides, and more than four out of every 10 were firearm homicides.
More people suffer nonfatal firearm-related injuries than die. More than seven out of every 10 medically treated firearm injuries are from firearm-related assaults. Nearly two out of every 10 are from unintentional firearm injuries. There are few intentionally self-inflicted firearm-related injuries seen in hospital emergency departments. Most people who use a firearm in a suicide attempt die from their injury.
Firearm injuries affect people in all stages of life. In 2020, firearm-related injuries were among the five leading causes of death for people aged 1 to 44 in the United States. Some groups have higher rates of firearm injury than others. Men account for 86% of all victims of firearm death and 87% of nonfatal firearm injuries. Rates of firearm violence also vary by age and race/ethnicity. Firearm homicide rates are highest among teens and young adults 15–34 years of age and among Black or African American, American Indian or Alaska Native, and Hispanic or Latino populations. Firearm suicide rates are highest among adults 75 years of age and older and among American Indian or Alaska Native and non-Hispanic White populations (CDC, 2024d).
The concentration of gun deaths across the U S with places like Los Angeles, Phoenix, New York, Washington, Ottawa, Mexico, and The Bahamas located on the map. The eastern and southeastern parts of the U S experience more gun deaths compared to other regions.
In contrast to the rising levels of gun violence in America, Europe has seen a decline in the homicide rate by 63% since 2002 and by 38% since 1990. The rate in Asia has fallen by 36% since 1990. There are also indications, however, that homicide is underreported in the official statistics in Pacific countries. Firearm suicide rates continued to remain high in the United States (United Nations Office on Drugs and Crime, 2018).
A comprehensive approach is needed to help reduce firearm-related deaths. Strategies that focus on underlying conditions can reduce disparities and the risk for violence while also strengthening protective factors at the individual, family, and community levels. Some actions can have a more immediate impact on preventing violence, and others can be long-term solutions. Prevention is a primary goal. Working with partners, including policymakers; local, state, territorial, and tribal governments; health, education, justice, and social service agencies; businesses; and community organizations can help ensure that local needs are met (CDC, 2022d; WHO, 2014). Gun violence intervention and prevention programs avert interpersonal violence by working with a range of community stakeholders to provide support and intervention to those at the highest risk of being persons who have been victimized and/or perpetrators of violence.
Additional Resources
- CDC – Fast Facts: Preventing Teen Dating Violence
- CDC – Injury and Violence Prevention [Video Playlist]
- CDC – Preventing Intimate Partner Violence Across the Lifespan: A Technical Package of Programs, Policies, and Practices [PDF]
- CDC, VetoViolence (tools and training, prevention information, ACEs resources)
- Disarm Domestic Violence (federal and state legislation and data)
- Gun Violence Archive
- TED Talk – How childhood trauma affects health across a lifetime (Nadine Burke Harris) [Video]
- Vera Institute for Justice – Screening for Human Trafficking: Guidelines for Administering the Trafficking Victim Identification Tool (TVIT) [PDF- Manual]
Resources for Patients/the Community
- 211 (information about local resources and services)
- Commonhelp.org (help with applying for assistance or health care)
- National Domestic Violence Hotline (also available at 1-800-799-SAFE)
- Virginia Department of Housing and Community Development – Housing Assistance
Chapter adapted from:
“Chapter Seven- Community Violence and Violence Prevention” by LibreTexts is licensed under CC BY.
